NAPA Programs Help “Second Victims” Recover from Adverse Clinical Events
NAPA REACH and Care for the Caregiver promote clinician wellness with peer support
by Deborah M. Barron, MD, Director, Care for the Caregiver, North American Partners in Anesthesia
During your clinical career have you ever been involved in an adverse event that you felt affected you mentally or emotionally? If you answered yes to this question, you may have experienced Second Victim Syndrome (SVS), and you are not alone. In fact, in a January 2018 Quick Safety advisory, The Joint Commission (TJC) cited a study estimating that nearly half of healthcare providers could experience the impact of being a second victim at least once in their career.1 More significantly for NAPA clinicians, a national survey conducted in 2012 concluded, “Most anesthesiologists will experience at least one perioperative catastrophe over the course of their careers.”2
The term “second victim” was first used in 2000 by Dr. Albert Wu, a professor at the Johns Hopkins School of Public Health, to describe healthcare providers who have been traumatized by their involvement in an unanticipated adverse patient event, medical error, and/or patient-related injury. Also known as “wounded healers” and “silent sufferers,” these providers, as the TJC noted, may experience the characteristics of post-traumatic stress disorder for months following an adverse event. Symptoms of fight or flight, anxiety, depression, flashbacks, loss of confidence, grief, and remorse may be compounded by concerns about trust from peers and the ongoing ability to practice. The sense of isolation that second victims typically feel is often made worse by workplace cultures that offer them no safety net or compassion.
The need to take better care of caregivers came to the forefront following the tragic suicide of Kimberly Hiatt, RN, which became international news in the summer of 2011. Hiatt had a spotless career at Seattle Children’s Hospital for 27 years when she accidentally administered an overdose of calcium chloride to a critically ill infant. Although she immediately acknowledged her error, she was subsequently fired and then battled to retain her nursing license. Seven months later, distraught at the death of her young patient and the prospect of losing the career she loved, Hiatt—a mother of two children herself—took her own life.
“Doctors have been taught how to counsel patients when an adverse outcome takes place, but unfortunately, they have not learned what to do for themselves under these circumstances,” wrote Dr. Arnold J. Berry in the spring 2006 issue of the Anesthesia Patient Safety Foundation’s APSF journal, dedicated to the topic of Dealing with Adverse Events.3
In the 2012 study, in which 82% of anesthesiologists reported being involved in a perioperative catastrophe, one in five clinicians claimed they have never recovered emotionally from the adverse event and one in eight considered changing careers. More than two-thirds of respondents felt compromised for the next four hours—even if they had to go back into the operating room—which raises the risk of “third victims”: patients who are subsequently harmed while the healthcare provider is still dealing with the aftermath of the first adverse event. But 98% felt that talking to a peer colleague about the event would have been helpful in their immediate and long-term recovery.
I believe taking care of our providers during one of the most vulnerable periods of their lives is essential to the wellness of any organization. As we began looking at our own NAPA community, we recognized that how you treat a provider immediately after a perioperative catastrophe says a lot about the culture of the site. NAPA has always had the Tier 3 Employee Assistance Program, but—consistent with national usage—fewer than 20% of our clinicians have taken advantage of the assistance in second victim instances. Overwhelmingly, at NAPA and nationwide, providers typically try to deal with their emotions on their own.
Because NAPA strives to promote an overall culture of clinician wellness in collaborative workplace environments, we began exploring how we could do better. First in this initiative was the creation of the NAPA Anesthesia Patient Safety Institute, which in December 2019 became a federally listed Patient Safety Organization (PSO). NAPA’s PSO status now protects all clinical conversations that are part of its Patient Safety Evaluation System, so that our providers can feel free to discuss adverse events with their clinical peers in confidence, without fear of legal repercussions, to review cases and possible lessons learned from the experience. A key goal of a PSO is to ensure that negative outcomes are reviewed and actions are taken to reduce events from reoccurring, which includes dissemination of educational lessons learned from case reviews in an effort to deliver safer patient care.
Next are two new programs designed specifically to encourage second victims to access assistance, which is then delivered quickly in the form of support by a trained peer colleague.
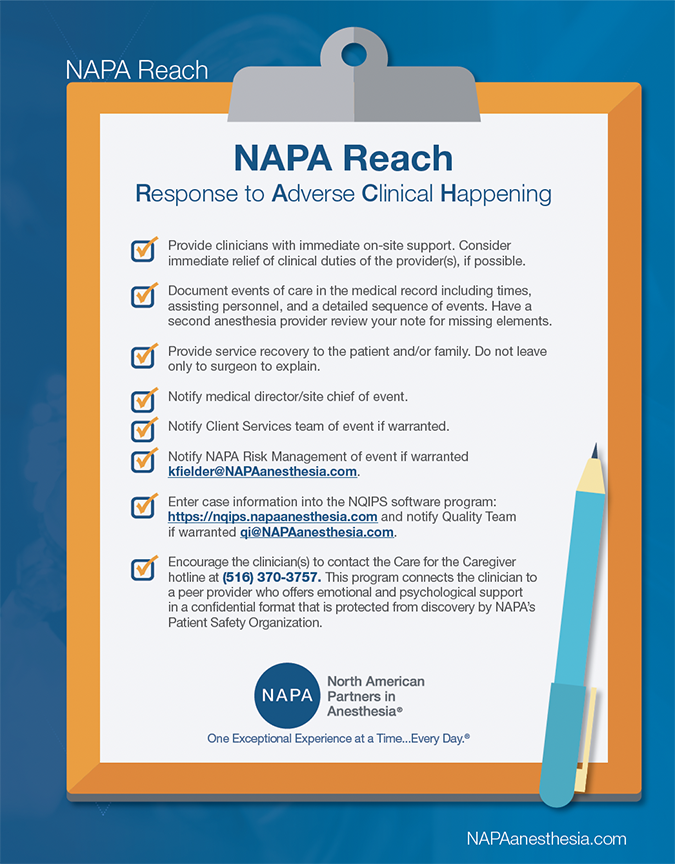
NAPA REACH (REsponse to an Adverse Clinical Happening)
The NAPA REACH checklist is a quick guide to steps that clinicians at any site should take following an adverse event. In addition to the usual notifications, the first guidance is to “Provide clinicians with immediate onsite support.”
After any adverse clinical happening, chiefs and colleagues are also advised to give the second victim a card that reminds them that “Whatever you’re feeling is a normal response to an abnormal event,” and to encourage the clinician to call NAPA Direct at (866) NAPA-HR1 to activate our second new program, Care for the Caregiver.
Care for the Caregiver
NAPA’s Care for the Caregiver program trains clinicians who volunteer to provide peer support to second victims. When a victim calls NAPA Direct after an adverse event and asks to activate Care for the Caregiver, a trained peer will be connected to the provider within a few hours to listen, help talk through the case, and offer emotional support. Our hope is that by giving second victims the opportunity to quickly speak with a trained peer in a PSO-protected environment, more clinicians involved in perioperative catastrophes will seek out and receive the timely help they need.
Care for the Caregiver is there for only one reason: to take care of the provider. NAPA’s patient-first philosophy requires us to take care of our clinicians, so our clinicians can deliver the best possible care to our patients. To me, this program exemplifies NAPA’s commitment to provider wellness, resilience, and integrity, and I am proud to share it with all our anesthesia physicians and CRNAs.
To my clinical colleagues throughout the company: I hope you never need these programs, but if you do, please reach out, call NAPA Direct, and ask to activate Care for the Caregiver. Please know that we are here for you.
1 The Joint Commission, Quick Safety, Issue 39, January 2018.
2 Gazoni FM, Amato PE, Malik ZM, Durieux ME, The impact of perioperative catastrophes on anesthesiologists: results of a national survey. Anesth Analg. 2012 Mar;114(3):596-603. doi: 10.1213/ANE.0b013e318227524e. Epub 2011 Jul 7.
3 Arnold J. Berry, MD, MPH, Adverse Events May Have Two Victims. APSF Newsletter, The Official Journal of the Anesthesia Patient Safety Foundation, Volume 21, No. 1, Spring 2006.